Eating Disorders And What Can Be Done?
Blue indicates link
Eating disorders are not just about food. They are often a way to cope with difficult problems or regain a sense of control. They are complicated illnesses that affect a person’s sense of identity, worth, and self-esteem.
When someone has an eating disorder, their weight is the prime focus of their life. Their all-consuming preoccupation with calories, grams of fat, exercise, and weight allows them to displace the painful emotions or situations that are at the heart of the problem and gives them a false sense of being in control.
What are eating disorders?
There are three main types of eating disorders: anorexia nervosa, bulimia nervosa, and binge-eating disorder.
Anorexia nervosa
A person who experiences anorexia nervosa may refuse to keep their weight at a normal weight for their body by restricting the amount of food they eat or exercising much more than usual. They may feel overweight regardless of their actual weight. They may think about their body weight often and use it to measure their self-worth.
Restricting food can affect a person’s entire body. Anorexia nervosa can cause heart and kidney problems, low blood iron, bone loss, digestive problems, low heart rate, low blood pressure, and fertility problems in women. As many as 10% of people who experience anorexia die as a result of health problems or suicide.
When you have anorexia, you excessively limit calories or use other methods to lose weight, such as excessive exercise, using laxatives or diet aids, or vomiting after eating. Efforts to reduce your weight, even when underweight, can cause severe health problems, sometimes to the point of deadly self-starvation.
Bulimia nervosa
Bulimia nervosa involves periods of uncontrollable binge eating, followed by purging (eliminating food, such as by vomiting or using laxatives). People who experience bulimia nervosa may feel overweight regardless of their actual weight. They may think about their body weight often and use it to measure their self-worth.
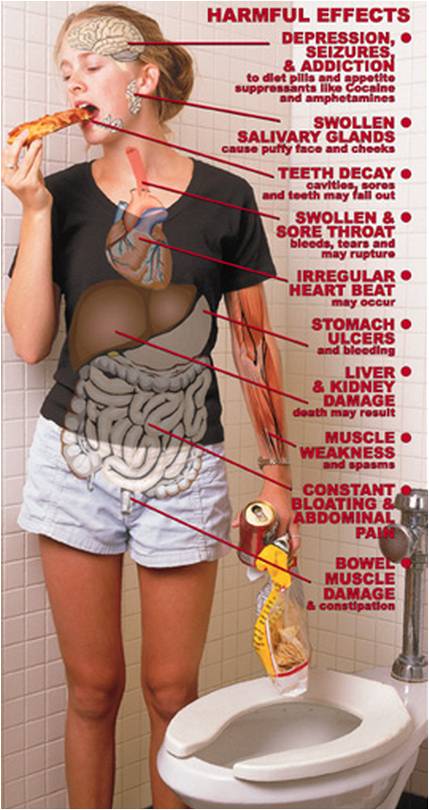
Health problems caused by bulimia nervosa may include kidney problems, dehydration, and digestive problems. Vomiting often can damage a person’s teeth, mouth, and throat.
If you have bulimia, you’re probably preoccupied with your weight and body shape and may judge yourself severely and harshly for your self-perceived flaws. You may be at a normal weight or even a bit overweight.
Binge-eating disorder
Binge-eating disorder involves periods of over-eating. People who experience binge-eating disorder may feel like they can’t control how much they eat and feel distressed, depressed, or guilty after bingeing. Many people try to keep bingeing a secret. Binge-eating can be a way to cope or find comfort, and it can sometimes develop after dieting. Some people may fast (not eat for a period of time) or diet after periods of binge-eating.
Binge-eating disorder can increase the risk of Type 2 diabetes, high blood pressure, or weight concerns.
After a binge, you may feel guilty, disgusted, or ashamed by your behavior and the amount of food eaten. But you don’t try to compensate for this behavior with excessive exercise or purging, as someone with bulimia or anorexia might. Embarrassment can lead to eating alone to hide your bingeing.
Personal Note:
I came into contact with these disorders when I was hospitalized for depression. I witnessed several beautiful young girls who felt they were overweight but you could actually see their bones, Anorexia. Still, other young women suffered from Bulimia. They would eat a full meal and feel guilty they ate so much, that they would make themselves throw up.
Who does it affect?
Eating disorders can affect anyone, but some people may be at higher risk. People who experience lower self-esteem poor body image, perfectionism, or difficulties dealing with stress may be more likely to experience an eating disorder. A lack of positive social support and other important connections may also play a big part. In some cases, eating disorders can go along with other mental illnesses.
Our beliefs about body image are also important. While the media may often portray thinness as an ideal body type, this alone doesn’t cause an eating disorder. How we think about those messages and apply them to our lives is what affects our self-esteem and self-worth.
What can I do about it?
You may have a lot of difficult feelings around finding help—it isn’t always an easy step to take. Many people who experience an eating disorder are scared to go into treatment because they may believe that they will have to gain weight. Many also feel a lot of shame or guilt around their illness, so the thought of talking about very personal experiences can seem overwhelming.
Some people find comfort in their eating behaviors and are scared to find new ways to cope. Restricting food, bingeing, and purging can lead to serious health problems, but eating disorders are treatable and you can recover. A good support team can help you through recovery and teach important skills that last a lifetime.
Treatment for an eating disorder usually involves several different health professionals. Some people may need to spend time in a hospital to treat physical health problems.
Counseling and support:
Counseling helps people work through problems and develop skills to manage problems in the future. There are different types of counseling, including cognitive-behavioral therapy, dialectical behavior therapy, and interpersonal therapy. The entire family may take part in counseling, particularly when a young person experiences an eating disorder.
It can be very helpful to connect with support groups. They’re an opportunity to share experiences and recovery strategies, find support, and connect with people who understand what you’re experiencing. There may also be support groups for family and friends affected by a loved one’s eating disorder.
There are many self-help strategies to try at home. Skills like problem-solving, stress management, and relaxation techniques can help everyone cope with challenges or problems in a healthy way. You’ll find many different skills like these in counseling, but you can practice them on your own, too. And it’s always important to spend time on activities you enjoy and connect with loved ones.
A dietitian or nutritionist can teach eating strategies and eating habits that support your recovery goals. This is also called ‘nutritional counseling.’
Medication:
While there are no medications specifically for eating disorders, medication may help with the mood problems that often go along with an eating disorder.
Medical care
Eating disorders can cause physical health problems, so you may need regular medical care and check-ups.
How can I help a loved one?
Supporting a loved one who experiences an eating disorder can be very challenging. Many people feel upset or even frightened by their loved one’s beliefs, behaviors, or state of well-being. An approach that focuses on support and understanding rather than control is best. Here are some tips to help you support a loved one:
- Remember that eating disorders are a sign of much bigger problems. Avoid focusing on food or eating habits alone.
- Be mindful of your own attitudes and behaviors around food and body image.
- Never force someone to change their eating habits or trick someone into changing.
- Avoid reacting to a loved one’s body image talk or trying to reason with statements that seem unrealistic to you.
- If your loved one is an adult, remember that supporting help-seeking is a balance between your own concerns and their right to privacy.
- If your loved one’s experiences are affecting other family members, family counseling may be helpful
- Don’t be afraid to set boundaries and seek support for yourself.
Rumination disorder:
Rumination disorder is repeatedly and persistently regurgitating food after eating, but it’s not due to a medical condition or another eating disorder such as anorexia, bulimia, or binge-eating disorder. Food is brought back up into the mouth without nausea or gagging, and regurgitation may not be intentional. Sometimes regurgitated food is re-chewed and re-swallowed or spit out.
The disorder may result in malnutrition if the food is spat out or if the person eats significantly less to prevent the behavior. The occurrence of rumination disorder may be more common in infancy or in people who have an intellectual disability.
Avoidant/restrictive food intake disorder:
This disorder is characterized by failing to meet your minimum daily nutrition requirements because you don’t have an interest in eating; you avoid food with certain sensory characteristics, such as color, texture, smell, or taste; or you’re concerned about the consequences of eating, such as fear of choking. Food is not avoided because of fear of gaining weight.
The disorder can result in significant weight loss or failure to gain weight in childhood, as well as nutritional deficiencies that can cause health problems.
When to see a doctor:
An eating disorder can be difficult to manage or overcome by yourself. Eating disorders can virtually take over your life. If you’re experiencing any of these problems, or if you think you may have an eating disorder, seek medical help.
Unfortunately, many people with eating disorders may not think they need treatment. If you’re worried about a loved one, urge him or her to talk to a doctor. Even if your loved one isn’t ready to acknowledge having an issue with food, you can open the door by expressing concern and a desire to listen.
Be alert for eating patterns and beliefs that may signal unhealthy behavior, as well as peer pressure that may trigger eating disorders. Red flags that may indicate an eating disorder include:
- Skipping meals or making excuses for not eating
- Adopting an overly restrictive vegetarian diet
- Excessive focus on healthy eating
- Making your own meals rather than eating what the family eats
- Withdrawing from normal social activities
- Persistent worry or complaining about being fat and talking about losing weight
- Frequent checking in the mirror for perceived flaws
- Repeatedly eating large amounts of sweets or high-fat foods
- Use of dietary supplements, laxatives, or herbal products for weight loss
- Excessive exercise
- Calluses on the knuckles from inducing vomiting
- Problems with loss of tooth enamel that may be a sign of repeated vomiting
- Leaving during meals to use the toilet
- Eating much more food in a meal or snack than is considered normal
- Expressing depression, disgust, shame, or guilt about eating habits
- Eating in secret
Causes:
The exact cause of eating disorders is unknown. As with other mental illnesses, there may be many causes, such as:
- Genetics and biology. Certain people may have genes that increase their risk of developing eating disorders. Biological factors, such as changes in brain chemicals, may play a role in eating disorders.
- Psychological and emotional health. People with eating disorders may have psychological and emotional problems that contribute to the disorder. They may have low self-esteem, perfectionism, impulsive behavior, and troubled relationships.
Remember you are beautiful just the way you are.
Risk factors:
Teenage girls and young women are more likely than teenage boys and young men to have anorexia or bulimia, but males can have eating disorders, too. Although eating disorders can occur across a broad age range, they often develop in the teens and early 20s.
Certain factors may increase the risk of developing an eating disorder, including:
- Family history. Eating disorders are significantly more likely to occur in people who have parents or siblings who’ve had an eating disorder.
- Other mental health disorders. People with an eating disorder often have a history of anxiety disorder, depression, or obsessive-compulsive disorder.
- Dieting and starvation. Dieting is a risk factor for developing an eating disorder. Starvation affects the brain and influences mood changes, rigidity in thinking, anxiety, and reduction in appetite. There is strong evidence that many of the symptoms of an eating disorder are actually symptoms of starvation. Starvation and weight loss may change the way the brain works in vulnerable individuals, which may perpetuate restrictive eating behaviors and make it difficult to return to normal eating habits.
- Stress. Whether it’s heading off to college, moving, landing a new job, or a family or relationship issue, change can bring stress, which may increase your risk of an eating disorder.
Complications:
Eating disorders cause a wide variety of complications, some of them life-threatening. The more severe or long-lasting the eating disorder, the more likely you are to experience serious complications, such as:
- Serious health problems
- Depression and anxiety
- Suicidal thoughts or behavior
- Problems with growth and development
- Social and relationship problems
- Substance use disorders
- Work and school issues
- Death
Prevention:
Although there’s no sure way to prevent eating disorders, here are some strategies to help your child develop healthy eating behaviors:
- Avoid dieting around your child. Family dining habits may influence the relationships children develop with food. Eating meals together gives you an opportunity to teach your child about the pitfalls of dieting and encourages eating a balanced diet in reasonable portions.
- Talk to your child. For example, there are numerous websites that promote dangerous ideas, such as viewing anorexia as a lifestyle choice rather than an eating disorder. It’s crucial to correct any misperceptions like this and to talk to your child about the risks of unhealthy eating choices.
- Cultivate and reinforce a healthy body image in your child, whatever his or her shape or size. Talk to your child about self-image and offer reassurance that body shapes can vary. Avoid criticizing your own body in front of your child. Messages of acceptance and respect can help build healthy self-esteem and resilience that will carry children through the rocky periods of their teen years.
- Enlist the help of your child’s doctor. At well-child visits, doctors may be able to identify early indicators of an eating disorder. They can ask children questions about their eating habits and satisfaction with their appearance during routine medical appointments, for instance. These visits should include checks of height and weight percentiles and body mass index, which can alert you and your child’s doctor to any significant changes.
If you notice a family member or friend who seems to show signs of an eating disorder, consider talking to that person about your concern for his or her well-being. Although you may not be able to prevent an eating disorder from developing, reaching out with compassion may encourage the person to seek treatment.
Anorexia Nervosa Statistics:
Anorexia Prevalence
- It is estimated that 1.0% to 4.2% of women have suffered from anorexia in their lifetime.
Anorexia Mortality Rates
- Anorexia has the highest fatality rate of any mental illness.
- It is estimated that 4% of anorexic individuals die from complications of the disease
Bulimia Nervosa Statistics:
Bulimia Prevalence
- It is estimated that up to 4% of females in the United States will have bulimia during their lifetime.
Bulimia Mortality Rates
- 3.9% of these bulimic individuals will die.
Binge Eating Disorder Statistics:
Binge Eating Prevalence
- 2.8 % of American adults will struggle with BED during their lifetime. Close to 43% of individuals suffering from Binge Eating Disorder will obtain treatment.
Binge Eating Disorder Mortality Rates
- 5.2% of individuals suffering from eating disorders not otherwise specified, the former diagnosis that BED, among other forms of disordered eating) was included in under the DSM-IV) die from health complications.
Female Eating Disorder Prevalence Rates:
- .9% of women will struggle with anorexia in their lifetime
- 1.5% of women will struggle with bulimia in their lifetime
- 3.5% of women will struggle with binge eating

Male Eating Disorder Statistics:
- .3% of men will struggle with anorexia
- .5% of men will struggle with bulimia
- 2% of men will struggle with binge eating disorder
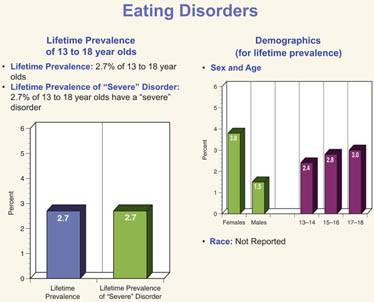
Prevalence Rates of Eating Disorders in Adolescents:
- The National Institute of Mental Health reports that 2.7% of teens, ages 13-18 years old, struggle with an eating disorder.
Student Eating Disorder Statistics:
- 50% of teenage girls and 30% of teenage boys use unhealthy weight control behaviors such as skipping meals, fasting, smoking cigarettes, vomiting, and taking laxatives to control their weight.
- 25% of college-aged women engage in bingeing and purging as a method of managing their weight.
Prevalence of eating disorders among athletes:
- 13.5% of athletes have subclinical to clinical eating disorders
- 42% of female athletes competing in aesthetic sports demonstrated eating-disordered behaviors
Dieting Statistics and Prevalence:
- Over 50% of teenage girls and 33% of teenage boys are using restrictive measures to lose weight at any given time.
- 46% of 9-11-year-olds are sometimes, or very often, on diets, and 82% of their families are sometimes, or very often, on diets).
- 91% of women recently surveyed on a college campus had attempted to control their weight through dieting, 22% often dieted or always.
- 95% of all dieters will regain their lost weight in 1-5 years.
- 35% of normal dieters progress to pathological dieting. Of those, 20-25% progress to partial or full syndrome eating disorders.
- 25% of American men and 45% of American women are on a diet on any given day.
Reference:
Anorexia Nervosa and Related Eating Disorders, Inc. website. Accessed Feb. 2012. http://www.anad.org/get-information/about-eating-disorders/eating-disorders-statistics/
Eating Disorders Statistics:
According to eating disorders statistics estimated by the National Eating Disorder Association, in the USA up to 30 million people suffer from an eating disorder such as anorexia nervosa, bulimia nervosa, or binge eating disorder. Worldwide the figure is more like 70 million sufferers!
The problem with statistics on eating disorders is that many sufferers do not come forward for diagnosis due to embarrassment, denial, or confusion as to what their symptoms are. Eating disorders can differ vastly in the expression of symptoms and behaviors, and just because a person does not fit into the DSM-5 classification does not mean that they do not have an eating disorder. DSM-5 is the manual used by mental health professionals in the U.S. to classify mental disorders.
Males are often one of the least diagnosed populations of people with eating disorders. This is probably due to shame about admitting to what is wrongly assumed to be a disorder that only affects women. For this reason, the number of men with eating disorders is probably much higher than the statistics claim.
Eating Disorders Statistics and Facts.
- Anorexia Nervosa has the highest mortality rate of any mental illness.
- An estimated 0.5 to 3.7 percent of women suffer from anorexia nervosa at some point in their lifetime. Research suggests that about 1 percent of female adolescents have anorexia.
- An estimated 1.1 to 4.2 percent of women have bulimia nervosa in their lifetime.
- The lifetime prevalence of binge eating disorder is 3.5% in women and 2.0% in men.
- The onset of anorexia nervosa is most commonly around the same time as puberty.
- Binge Eating Disorder was found to usually start during late adolescence or in the early twenties.
- A study in 2003 found that people with anorexia are 56 times more likely to commit suicide than non-sufferers.
- Alcohol and substance abuse are four times more prevalent among people who suffer from eating disorders.
- Hospitalizations for eating disorders in children under the age of 12 years old increased by 119 percent between the years of 1999 and 2006.
- Twin studies show that there is a significant genetic component to eating disorders.
- In childhood (5-12 years), the ratio of girls to boys diagnosed with AN or BN is 5:1, whereas, in adolescents and adults, the ratio is much larger – 10 females to every one male.
- Young women with anorexia are 12 times more likely to die than other women the same age that doesn’t have anorexia.
- The most common eating disorder in the United States is binge eating disorder (BED). It is estimated that 3.5% of women, 2% of men, and 30% to 40% of those seeking weight loss treatments can be clinically diagnosed with binge eating disorder.
Statistics and Facts on Dieting and Disordered Eating.
Disordered eating is different from an eating disorder. A person who worries about their looks and as a result, their eating patterns are disrupted but does not have an eating disorder, might fall into this category.
- 51% of girls 9 and 10 years old feel better about themselves when they are dieting.
- A 2002 study of boys in grades 9 and 10 found that 4% of them reported anabolic steroid use. This shows that body preoccupation and efforts to change one’s body are concerns that affect both women and men.
- 40% of girls in grade ten and 37% of girls in grade nine thought of themselves as being too fat. Of those students who were “normal weight” based on their BMI, 19% still thought that they were too fat, and 12% of the students admitted to trying to lose weight.
- Body-based bullying can have a severe impact on a girl’s attitude and behavior. Girls who suffered teasing by members of their families were 1.5 times more likely to try binge eating and/or other dangerous weight-control methods within five years.
- 91% of women who were surveyed on a college campus had tried to control their weight by dieting, and 22% of them dieted “often” or all the time.
Statistics on Eating Disorders Recovery:
- With treatment, 60% of eating disorder sufferers make a full recovery.
- Without treatment, 20% of people suffering from anorexia will prematurely die from eating disorder-related health complications, including suicide and heart problems.
- Inpatient treatment of an eating disorder in the US ranges from $500 – $2,000 per day. Long-term outpatient treatment, including therapy and medical monitoring, can cost $100,000 or more. Thankfully insurance companies now usually cover eating disorder treatment.
- Only one in ten sufferers will seek and receive treatment.
- Treatment is most successful when intervention is early.
- Eating disorders statistics tell us that in order for treatment to be successful, it must be multifaceted. It must include medical care, mental health care, and nutritional education and counseling.
- Long-term treatment is often needed; eating disorders require ongoing care.
Is There a Cure for Eating Disorders?
No simple cure exists for eating disorders, but treatment is available, and recovery is possible. Through a combination of therapy, nutritional education, and medical treatment, the symptoms of an eating disorder can be managed or eliminated. Unfortunately, only one in 10 people with an eating disorder receive treatment, but true recovery is possible. Early diagnosis and treatment significantly increase your chances of recovery, so if you or someone you love is battling an eating disorder, call to explore available treatment options.
Many people do not need medications for eating disorders during treatment, but eating disorder medications are needed in some cases. When they are used, it’s important that they be only part of a treatment plan; there is no magic cure for eating disorders. Patients also need to be aware that all eating disorder medications come with side effects and the risks of the drug need to be evaluated against the potential benefit.
These medications are primarily prescribed to stabilize the patient both mentally and physically. Eating disorder medications include:
Electrolytes
Electrolytes include:
-
-
- Potassium chloride
- Calcium gluconate
- Potassium phosphate
-
- Common psychiatric eating disorder medications include the following types:
-
- Selective serotonin reuptake inhibitors (SSRI): These antidepressants have the strongest evidence as eating disorder medications with the fewest side effects. In addition to fluoxetine, examples of SSRIs include sertraline and fluvoxamine (Luvox).
- Tricyclic antidepressants (TCAs) and monoamine oxidase inhibitors (MAOIs): These older antidepressants have some evidence of being effective in eating disorders treatment; however, they have more side effects than SSRIs. An example is imipramine (Tofranil).
- Other antidepressants: Other antidepressants are also used in the treatment process. Examples are bupropion (Wellbutrin) and trazodone (Desyrel)
- Mood stabilizers: There is some evidence for using mood stabilizers to treat eating disorder patients. Because mood stabilizers can have adverse effects such as weight loss, mood stabilizers are not the first choice for eating disorder medications. Examples of mood stabilizers are topiramate (Topiramate) and lithium.
- “Other” medications
- Orlistat (Xenical): an anti-obesity drug
- Ephedrine and caffeine: stimulants; energizing drugs
- Methylphenidate: typically used when attention deficit hyperactivity disorder accompanies the eating disorder
- Medications for co-existing medical and/or mental health conditions.
Personal Note:
I fear some of the drugs listed above. Please research the drug you are prescribed. Side effects may be nasty.
I am not a Doctor. Please always follow your doctor’s recommendations.
Know Your Options:
Where to start?
Whether you start by seeing your primary care practitioner or some type of mental health professional, you’ll likely benefit from a referral to a team of professionals who specialize in eating disorder treatment. Members of your treatment team may include:
- A mental health professional, such as a psychologist to provide psychological therapy. If you need medication prescription and management, you may see a psychiatrist. Some psychiatrists also provide psychological therapy.
- A registered dietitian to provide education on nutrition and meal planning.
- Medical or dental specialists to treat health or dental problems that result from your eating disorder.
- Your partner, parents, or other family members. For young people still living at home, parents should be actively involved in treatment and may supervise meals.
It’s best if everyone involved in your treatment communicates about your progress so that adjustments can be made to treatment as needed.
Managing an eating disorder can be a long-term challenge. You may need to continue to see members of your treatment team on a regular basis, even if your eating disorder and related health problems are under control.
Setting up a treatment plan:
You and your treatment team determine what your needs are and come up with goals and guidelines. Your treatment team works with you to:
- Develop a treatment plan. This includes a plan for treating your eating disorder and setting treatment goals. It also makes it clear what to do if you’re not able to stick with your plan.
- Treat physical complications. Your treatment team monitors and addresses any health and medical issues that are a result of your eating disorder.
- Identify resources. Your treatment team can help you discover what resources are available in your area to help you meet your goals.
- Work to identify affordable treatment options. Hospitalization and outpatient programs for treating eating disorders can be expensive, and insurance may not cover all the costs of your care. Talk with your treatment team about financial issues and any concerns — don’t avoid treatment because of the potential cost.
Psychological therapy:
Psychological therapy is the most important component of eating disorder treatment. It involves seeing a psychologist or another mental health professional on a regular basis.
Therapy may last from a few months to years. It can help you to:
- Normalize your eating patterns and achieve a healthy weight
- Exchange unhealthy habits for healthy ones
- Learn how to monitor your eating and your mood
- Develop problem-solving skills
- Explore healthy ways to cope with stressful situations
- Improve your relationships
- Improve your mood
Treatment may involve a combination of different types of therapy, such as:
- Cognitive-behavioral therapy. This type of psychotherapy focuses on behaviors, thoughts, and feelings related to your eating disorder. After helping, you gain healthy eating behaviors, it helps you learn to recognize and change distorted thoughts that lead to eating disorder behaviors.
- Family-based therapy. During this therapy, family members learn to help you restore healthy eating patterns and achieve a healthy weight until you can do it on your own. This type of therapy can be especially useful for parents learning how to help a teen with an eating disorder.
- Group cognitive-behavioral therapy. This type of therapy involves meeting with a psychologist or other mental health professional along with others who are diagnosed with an eating disorder. It can help you address thoughts, feelings, and behaviors related to your eating disorder, learn skills to manage symptoms and regain healthy eating patterns.
Your psychologist or other mental health professionals may ask you to do homework, such as keep a food journal to review in therapy sessions and identify triggers that cause you to binge, purge, or do other unhealthy eating behaviors.
Nutrition education:
Registered dietitians and other professionals involved in your treatment can help you better understand your eating disorder and help you develop a plan to achieve and maintain healthy eating habits. The goals of nutrition education may be to:
- Work toward a healthy weight
- Understand how nutrition affects your body, including recognizing how your eating disorder causes nutrition issues and physical problems
- Practice meal planning
- Establish regular eating patterns — generally, three meals a day with regular snacks
- Take steps to avoid dieting or bingeing
- Correct health problems that are a result of malnutrition or obesity
Natural Remedies and Herbs for Eating Disorders:
- Chamomile – This is a tea that has natural soothing and calming benefits that reduce anxiety which may be an eating disorder cause.
- St. John’s Wort – St. John’s Wort is a natural plant that increases serotonin levels and alleviates the stress associated with eating disorders.
- Ginger – A known appetite stimulant, ginger can be effective in treating anorexia. It’s best consumed with lemon juice and rock salt on an empty stomach.
- Probiotics – These are essential supplements to help improve nutritional deficiencies and are highly efficient in treating anorexia.
- Ashwagandha – Ashwagandha is a natural herb remedy taken for depression and eating disorders. It helps boost energy levels and increases appetite.
- Passion Flower – This herbal remedy is derived from a climbing vine and is used to treat personality and anxiety issues. It increases the levels of brain chemicals known as gamma-aminobutyric acid (GABA).
Alternative treatments for eating disorders: the role of yoga:
Yoga helps in the reduction of stress levels and also enhances clearer thinking. Exercise done in yoga is of low impact and allows people to get in tune with their bodies. A particular study showed that women witnessed significant changes in:

- Their sense of well-being and positive feelings
- Reduced self-objectification
- A reduction in poor eating habits
- More positive body image
BED-Related Depression And Saffron Extract Treatment:
Saffron extract may reduce serotonin reuptake in the synapses. This synaptic serotonin reuptake inhibition retains the mood-elevating neurotransmitter in the brain for a longer duration, boosting its impact and reducing depression. Saffron extract has antioxidant and anti-inflammatory effects that hold therapeutic potential for a lot of nervous system disorders.
An animal study additionally showed that many parts of the saffron plant contain antidepressant properties. The saffron extract helps to combat mild to moderate depression and anxiety, which triggers binge eating. Saffron is an effective therapy for the treatment of mild to moderate depression and it may be as effective as fluoxetine.
St John’s Wort:
There are many scientific pieces of evidence that St John’s wort may reduce symptoms in people with mild-to-moderate, but not severe depression. Thus, it can be useful in the treatment of binge eating disorder-related depression. Some studies found that it has a similar function as selective serotonin reuptake inhibitors (SSRIs), a well-accepted form of antidepressant frequently prescribed for the treatment of depression.
Thus, the herb St John’s Wort presents another natural and herbal treatment to treat binge eating disorder and a way to raise serotonin levels. It is a natural serotonin booster that helps to lessen anxiety and depression.
Serotonin is a chemical in the brain responsible for feeling good and connected with mood, appetite, sleep, learning, and memory. If your serotonin levels are too low, you are likely to be anxious and perceive the world as unfriendly.
Before using John’s wort, you must be aware that there are potential risks of interactions of John’s worth with other related prescribed medications and drugs that treat binge eating disorder. Talk to your healthcare provider before using St John’s wort if you are also using other medications.
5-HTP:
5-HTP is another natural supplement that boosts serotonin and reduces anxiety and depression. Consult your doctor if you are taking any other antidepressant medication or serotonin booster before taking this supplement.
L-Tryptophan For Anxiety
Although l-tryptophan can be obtained from your diet, and especially a therapeutic eating plan for binge eating disorder recovery, a number of people choose to take a more direct approach to obtain additional tryptophan and boost serotonin levels. L-Tryptophan is available as a supplement and helps to treat depression, though it does require a doctor’s prescription.
Vitamin Supplements:
The daily intake of vitamin supplements that are made up of vitamins A, B, C, and E and minerals like calcium, magnesium, and potassium are essential in activating brain function and stabilizing the appetite. Foods rich in omega-3 fatty acids boost the relaxation of muscles and help to minimize stress.
A multivitamin supplies the body with the necessary nutrition and sustains a chemical balance. Together with therapy for binge eating disorder, it can help you control your urge to binge eat.
Supplements That Boost Dopamine Levels:
Dopamine is a neurotransmitter responsible for motivation. It is usually injected intravenously and easily reaches the brain this way. There are a number of herbs, amino acids, and natural compounds that naturally boost the levels of dopamine in the brain.
Some of these supplements are used for specific psychological issues like ADHD, depression, or anxiety, and we’ll discuss some of those now.
L-Tyrosine:
The top recommended dopamine supplement is l-tyrosine. L-tyrosine is an amino acid that acts as a precursor to dopamine. Tyrosine is naturally present in protein-rich foods like animal products and legumes. If your diet is deficient in l-tyrosine, you will have insufficient dopamine. There are many forms of tyrosine supplements but the best of them all is the highly absorbable form of l-tyrosine that acts as a filter that keeps foreign substances out of the brain.
Mucuna Pruriens:
Mucuna pruriens is a tropical legume that is also referred to as velvet bean or cowhage. The beans and pods are made up of l-dopa, a dopamine precursor. Mucuna pruriens supplements help to boost mood, memory, and general brain health. Research shows that Mucuna pruriens is more functional than levodopa medications.
Phosphatidylserine:
Phosphatidylserine (PS) is a popular natural brain supplement that boosts dopamine levels and helps to improve memory, concentration, and symptoms of ADHD. It also reduces levels of the stress hormone cortisol. Phosphatidylserine can be obtained in food like cow brains and chicken hearts.
Ginkgo Biloba:
Ginkgo biloba is another popular herbal remedy for brain-related disorders like depression and anxiety.
L-Theanine:
L-theanine is an amino acid that is present in green tea. L-Theanine increases dopamine and boosts mood.
SAM-e:
SAM-e (s-adenosyl methionine) is a natural remedy for depression. It boosts the levels of dopamine, serotonin, and other neurotransmitters that are responsible for a good mood.
Essential Body Awareness Therapy:
A study found that essential body awareness therapy can help to manage binge eating disorder. Body awareness therapy centers on awareness of some valuable movements. This treatment helped individuals with binge eating disorders to increase self-awareness.
Yoga Therapy:
Yoga helps your binge eating by minimizing your stress levels. A study showed that women who practice yoga improved their positive feelings and a sense of worth significantly. They also showed improved body image, reduced self-objection, and better eating habits.
Another study found that home yoga when practiced together with regular formal weekly sessions, helps in the treatment of binge eating disorder.
Acupuncture Therapy:
Acupuncture together with regular treatments of binge eating disorder, can be effective in minimizing symptoms of depression, gives individuals a better sense of control, and improves their mental and physical health.
Relaxation Therapy:
Massage and relaxation therapy helps to improve patients’ personal attitude to life which makes it easier for them to recover. Massage therapy boosts the levels of serotonin and dopamine and lessens levels of depression, anxiety, and stress that trigger binge-eating episodes.
Relaxation therapies like aromatherapy and meditation help to minimize emotional binge eating, boost self-acceptance, and help the individual discover binge eating triggers. Research shows that these therapies also curb anxiety, and food addiction, and help the patient’s ability to manage pain.
Biofeedback:
A pilot study discovered that individuals with varying types of eating disorders found heart rate variability (HRV) biofeedback very helpful in combating their eating disorders.
Biofeedback is the process of gaining greater awareness of many physiological functions of one’s own body, primarily using electronic or other instruments, with the goal of being able to manipulate the body’s systems at will. Some of the processes that can be controlled include brainwaves, muscle tone, skin conductance, heart rate, and pain perception.
Biofeedback may be used to improve health, performance, and physiological changes that often occur in conjunction with changes to thoughts, emotions, and behavior. Eventually, these changes may be maintained without the use of extra equipment, for no equipment is necessarily required to practice biofeedback.
Biofeedback has been found to be effective for the treatment of headaches and migraines.
Personal Note:
Please do not compare yourselves to some of the images you may see from Hollywood or certain models. That stereotype is changing. You look great, believe in yourself, and be your own best friend.
Thank you for reading.
Michael.
Comments are welcome
Hi! Thank you for this thorough post. It’s really sad to read about all the different types of eating disorders. But in order to help a person we love to overcome the issue we need to put ourselves in their shows and know a bit more about the disorder they’re suffering.
Hi Henry,
Thank you for your comments. You are so right sometimes to understand someone we have to put ourselves in their shoes.
Best wishes,
Michael
Hey, I enjoy a low while reading your article on Eating disorders symptoms effects and find it very useful for me. My grand father have the eating disorder problem. Your step by step guide is very helpful to understand it in better way. Now we are doing Acupuncture Therapy & Relaxation Therapy both are working good. Now I know that massage and relaxation therapy helps to improve patients’ personal attitude to life which makes it easier for them to recover. Your guide is very helpful for everyone.
Hi Harish,
Thank you for your comments. I hope your grand father is doing well with the therapy.
Best wishes,
Michael